
WI DPH 7119 2001-2024 free printable template
Show details
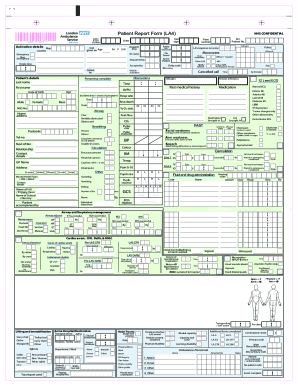
DEPARTMENT OF HEALTH & FAMILY SERVICES Division of Public Health DPH 7119 (Rev. 02/01) Mo/Day/Yr Completion of this form meets the requirements of administrative rule HFS 110.04(3)(b). Some client
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign

Edit your patient report form ambulance form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your patient report form ambulance form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient report form ambulance pdf online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit patient report form pdf. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
How to fill out patient report form ambulance

How to fill out patient report form ambulance:
01
Make sure to accurately record the patient's personal information, including their name, address, and phone number.
02
Document the date and time of the incident or emergency, as well as the location where it occurred.
03
Provide a detailed description of the patient's condition, including any symptoms they are experiencing and the severity of their injuries or illness.
04
Include relevant medical history, such as any existing conditions or allergies that may impact the treatment provided.
05
Record the vital signs of the patient, including their heart rate, blood pressure, and respiratory rate.
06
Describe any treatments or procedures performed by the medical personnel, including medications administered and any tests conducted.
07
Document the patient's response to the treatment and any changes in their condition during transport.
08
Finally, ensure that the form is signed and dated by the medical personnel responsible for the patient's care.
Who needs the patient report form ambulance:
01
Emergency medical personnel who responded and provided treatment to the patient.
02
Hospital staff who will take over the patient's care upon arrival.
03
Insurance companies or government agencies that may require the patient report for reimbursement or legal purposes.
Video instructions and help with filling out and completing patient report form ambulance pdf
Instructions and Help about electronic patient report form
Fill ambulance report pdf : Try Risk Free
People Also Ask about patient report form ambulance pdf
What is a patient report form?
How do you write a patient report?
What should a patient report include?
How do you write a soap note in EMS?
How do you write a patient report for EMS?
What is a patient report?
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Who is required to file patient report form ambulance?
The patient report form must be filed by the ambulance service or provider that transported the patient.
How to fill out patient report form ambulance?
1. Patient Information:
-Name:
-Address:
-Phone Number:
2. Transport Information:
-Mode of Transport: Ambulance
-Location of Pickup:
-Time of Pickup:
-Location of Destination:
3. Medical Information:
-Type of Injury/Illness:
-Symptoms Noted:
-Vital Signs Recorded:
4. Treatment Provided:
-Medication Administered:
-Procedures Performed:
-Other Treatment Provided:
5. Additional Notes:
-Notes on Patient Condition:
-Notes on Treatment Provided:
-Notes on Transport:
What is the purpose of patient report form ambulance?
The purpose of a patient report form for an ambulance is to provide a clear and concise record of a patient's medical history, condition, and treatment. This information can be used to help medical personnel make decisions about how best to treat the patient, as well as to provide documentation of the care given for legal and insurance purposes.
What information must be reported on patient report form ambulance?
1. Patient's name, age, and gender
2. Date and time of the call
3. Location of the call
4. Chief complaint and any other relevant medical history
5. Vital signs (blood pressure, temperature, pulse, respiration rate, oxygen saturation)
6. Treatment provided during transport (medications, oxygen, etc.)
7. Destination of the transport
8. Mode of transport used (ground or air ambulance)
9. Patient's condition on arrival and departure
10. Patient's final destination and outcome of the transport
What is the penalty for the late filing of patient report form ambulance?
It is difficult to answer this question without more information. Penalty amounts and types of penalties vary by jurisdiction. For example, in the UK, late filing of patient reports can result in fines or other disciplinary action from the Health and Care Professions Council, while in the US, penalties may vary by state.
What is patient report form ambulance?
A patient report form in an ambulance or pre-hospital setting is a document that is used to record important information about a patient's condition, vital signs, medical history, interventions performed, and other relevant details during the course of their care. This form serves as an important communication tool between healthcare providers and can be used for proper documentation, continuity of care, and accountability. The details included in the patient report form may vary depending on local protocols and policies.
How can I send patient report form ambulance pdf to be eSigned by others?
patient report form pdf is ready when you're ready to send it out. With pdfFiller, you can send it out securely and get signatures in just a few clicks. PDFs can be sent to you by email, text message, fax, USPS mail, or notarized on your account. You can do this right from your account. Become a member right now and try it out for yourself!
How do I complete ambulance report form on an iOS device?
pdfFiller has an iOS app that lets you fill out documents on your phone. A subscription to the service means you can make an account or log in to one you already have. As soon as the registration process is done, upload your patient report form template. You can now use pdfFiller's more advanced features, like adding fillable fields and eSigning documents, as well as accessing them from any device, no matter where you are in the world.
How do I edit patient report form on an Android device?
You can make any changes to PDF files, like patient report form examples, with the help of the pdfFiller Android app. Edit, sign, and send documents right from your phone or tablet. You can use the app to make document management easier wherever you are.
Fill out your patient report form ambulance online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Ambulance Report Form is not the form you're looking for?Search for another form here.
Keywords relevant to ambulance prf example form
Related to patient report form ambulance





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
